HBOT Conversations:
Tom Fox (Part 1)
Tom is the Research Physiologist for the Hyperbaric Institute for Research and Training, a division of Island Hyperbaric Centre in Pincourt QC. He has worked in the field of Clinical Hyperbaric Oxygen for the last 30 years, and has been intimately involved with the implementation and the development of the US Army’s Clinical Hyperbaric Service at Dwight David Eisenhower Army Medical Center. Tom is a senior army aviator and flew twelve years as a Medical Evacuation Pilot for the US Army.
Tom joined the Extivita-RTP team in 2022 as the Safety Director, and is joining us in a 2-part series to discuss the history of Hyperbaric Oxygen Therapy and dive into his personal experience healing patients with HBOT.
Watch the Podcast
We appreciate HBOT historian, Tom Fox, returning to HBOT News to dive in deeper to the history of Hyperbarics, which we can date back to the 1660s!
Tom explains that in the 1830s, the first clinical use of hyperbarics was used and introduced, this revived Nathaniel Henshaw’s concept of Hyperbaric treatments. Nathaniel Henshaw, a clergyman, built a sealed chamber in 1662. Henshaw believed that the application of higher pressure (hyperbaria) was good to treat acute conditions, and that lower pressure (hypobaria) would be better to treat chronic diseases.
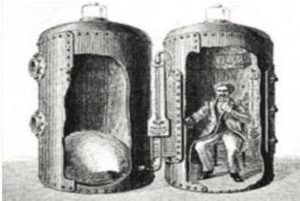
1662, Henshaw’s “Domicilium” hyperbaric chamber
This is an interesting fact, because now we’re learning that the cyclic use of hyperbaria (or relative hyperbaria) and hypobaria is very intriguing in what it’s doing from the standpoint of physiology. Tom mentions Dr. Efrati and his group of researchers have been at the forefront of looking at this, and are doing a phenominal job of conducting the hyperbaric studies and getting the hyperbaric education out there. There’s been very limited commitment to do this, he commends Dr. Efrati and his group at Tel Aviv for all they do for the HBOT industry. What you will witness throughout the history of hyperbarics is that they’ve used slightly pressurized room air, and that’s important to know because the slightly pressurized room air has consistently been assumed not to have any effect. It’s even offered up as a control in many of the studies, like the placebo. But the problem is when the placebo helps and the treatment helps, it’s easy to say that the reason both groups are getting better is because of the “participation effect”, or it being “in their heads”. And Dr. Efrati is bringing all this to light. This information is also changing the way the HBOT industry looks at the application of air breaks within the protocols. The use of air breaks was thought to fight oxygen toxicity, but now it’s used to establish a relative hypoxia without going into hypoxic conditions. Host di Girolamo then breaks all of that information down for the viewer to better understand…
So to paraphrase that, you’re breathing pure oxygen and also now you’re breathing air, your body says, ‘oh, oxygen’s depleting, you’re suffocating.’ All these mechanisms occur in your physiology, and then the body’s like, ‘Oh, no, everything’s okay. We have plenty of oxygen.’ So that five minute air break triggers that, and then he’s doing it, I think, three or four times in a 90 minute treatment and it ends up being therapeutic.
Continuing down the timeline of HBOT and fascinating discoveries in the 1800s, Tom Fox brings up a series of articles, Lectures on The Compressed Air Bath and its uses in the treatment of disease, that appeared in the British Medical Journal, dated April 18th, 1885 by a doctor, Theodore Williams. Tom reads the first paragraph from the first article:
“The use of atmospheric air under different degrees of barometric pressure in the treatment of disease is one of the most important advances in modern medicine. When we consider the simplicity of the agent, the exact method by which it is applied, and the precision with which it can be regulated to the requirements of each individual, we are astonished that in England, this method of treatment has been so little used.” – Theodore Williams
That was almost 150 years ago. Back then they were just taking air and putting you under pressure. Now it’s a breakthrough medical treatment, and it’s still not being used in the manner that it could/should be. Almost 200 years ago we were on the cutting edge of medicine! And today we still have to fight to explain that even slightly pressurized room air has a therapeutic benefit — using pressure for healing purposes has literally been happening since the 1600s.
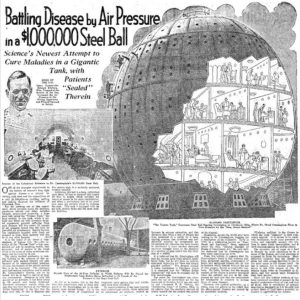 Now we approach the 1900s in the HBOT history timeline. One of the most famous (and LARGEST) chambers is discussed, the Cunningham Ball, by Dr. Cunningham. Dr. Cunningham clearly saw the benefits of Hyperbaric Oxygen Therapy and basically risked his entire career/life, and life savings to help people and prove the benefits. Doctor Cunningham was an anesthesiologist by trade, inventing circuits that are still in use and still patented by anesthesiology. In the 1918s, with the last pandemic of the Spanish Flu, Dr. Cunningham made the observation that there was a higher mortality rate when you went to Denver, as opposed to when you were at sea level, because of the pressure and oxygen changes. Ultimately a Spanish Flu patient in Denver was getting a lower dose of oxygen because of the lower air pressure. Dr. Cunningham even saved the life of one gentleman who was turning blue by simply treating with hyperbaric air. This lead to the dedication of $1M in funds to build the famous Cunningham ball, which was almost like a pressurized six story hotel that people would live in for a month or other extended periods of time.
Now we approach the 1900s in the HBOT history timeline. One of the most famous (and LARGEST) chambers is discussed, the Cunningham Ball, by Dr. Cunningham. Dr. Cunningham clearly saw the benefits of Hyperbaric Oxygen Therapy and basically risked his entire career/life, and life savings to help people and prove the benefits. Doctor Cunningham was an anesthesiologist by trade, inventing circuits that are still in use and still patented by anesthesiology. In the 1918s, with the last pandemic of the Spanish Flu, Dr. Cunningham made the observation that there was a higher mortality rate when you went to Denver, as opposed to when you were at sea level, because of the pressure and oxygen changes. Ultimately a Spanish Flu patient in Denver was getting a lower dose of oxygen because of the lower air pressure. Dr. Cunningham even saved the life of one gentleman who was turning blue by simply treating with hyperbaric air. This lead to the dedication of $1M in funds to build the famous Cunningham ball, which was almost like a pressurized six story hotel that people would live in for a month or other extended periods of time.
Apparently, Cunningham had some difficulty justifying it all by scientific standards, and this was a very new concept in US medicine. The world had never seen anything like it! Unfortunately, Cunningham fell victim toa unusual amount of scrutiny, and was eventually shut down with the chamber being sold for scrap metal during World War II.
So many people now see the value in Cunningham’s efforts and what he contributed to the HBOT industry. Finally, his work can be interpreted as vindication of the God-given miracle of oxygen and pressure to heal our bodies and minds.
Guests

Thomas M. Fox, MAS,MS, CHT - Safety Director at Extivita RTP & Research Physiologist for the Hyperbaric Institute for Research and Training
Tom is the Research Physiologist for the Hyperbaric Institute for Research and Training, a division of Island Hyperbaric Centre in Pincourt QC. He has worked in the field of Clinical Hyperbaric Oxygen for the last 30 years. During this time, he has been intimately involved with the implementation and the development of the US Army’s Clinical Hyperbaric Service at Dwight David Eisenhower Army Medical Center. He has provided contract hyperbaric services since 1997. Prior to accepting his current position in Quebec, Canada, Mr. Fox served as the Chief of the Atmospherics Branch of the U.S. Army School of Aviation Medicine, Fort Rucker Alabama. In this capacity, he was responsible for hyperbaric/ hypobaric operations and training of US and NATO aviators, flight surgeons and flight medics. Mr. Fox is a senior army aviator and flew twelve years as a Medical Evacuation Pilot for the US Army.
Tom joined the Extivita team in 2022 as the Safety Director, helping Extivita to maintain a healthy and safe environment for exceptional patient care.
Subscribe Now, It’s Free!
Recent HBOT News
Clinical Trial – Transcranial Magnetic Stimulation and Hyperbaric Chamber for Women Fibromyalgia
Fibromyalgia syndrome (FMS) is a multisystem disease, characterized by generalized chronic
musculoskeletal pain. In addition, there is a lot of care for fatigue, sleep disorders,
morning stiffness, cognitive disorders, depression, anxiety and stress. Other common symptoms
are back pain, headaches, irritable bowel, balance problems and deterioration of physical
function in general. Patients with fibromyalgia (FM) often show pain at specific points that
are known as "tender spots or tender spots, with an increased sensitivity to painful stimuli"
(hyperalgesia) and a decreased pain threshold (allodynia). which can be evidenced in the
physical examination and in the absence of anomalies that justify in the biological or image
tests. These pain points to pressure, based on the most specific and specific criteria for
the diagnosis of the disease, traditionally based on the criteria of the American College of
Rheumatology (ACR), according to which, should be presented so minus 11 out of 18 painful
points to confirm it. Although the etiology remains unknown and unclear, its appearance is
attributed to a problem of central sensitization, that is, changes in central processing,
which causes an alteration of the mechanisms that regulate the sensation of pain, with
amplification of nociceptive input . and perpetuation of painful stimuli. Fibromyalgia is
becoming a common syndrome in the countries of Western Europe, with a prevalence in the
general population that ranges between 1-3%, and specifically in Spain, around 2.4%. In
addition, it has a higher incidence in women than men (73-95%), predominantly affecting women
between the ages of 40-50 years. About 3% of women with fibromyalgia are at an age when
menopause occurs, so not only do they experience the symptoms of both states but they even
exacerbate the syndrome with each other. On the other hand, and in relation to its
chronicity, the care of this type of patients involves large costs for society with a
significant consumption of health resources in the field of primary care, as well as the
costs of work absenteeism. For these reasons, it is considered an important problem with a
great impact on the health system, and therefore more and more studies are being developed
with the aim of better understanding the pathophysiology of this disease. The therapeutic
approach includes low cost and easy access measures, such as physical exercise (EF) programs
to improve the symptoms of FM. Physical exercise has positive effects directly on pain, joint
and muscle stiffness, generalized sensitivity and fatigue, among others, and secondarily on
cognitive disorders. Thus, the vast majority of studies focus on low-impact aerobic exercise,
performed between 60% and 70% of the maximum heart rate two to three times a week. However,
to date, there is no study that compares the effectiveness of physical exercise with other
innovative therapeutic actions, such as transcranial magnetic stimulation (TMS), the
hyperbaric chamber (HBOT), in parameters related to pain and quality of life. the life of
patients with fibromyalgia. The general objective is the effectiveness of transcranial
magnetic stimulation and the hyperbaric chamber in women with fibromyalgia. As specific
objectives we propose:
To assess the effect of HBOT, TMS and EF on quality of life in women with fibromyalgia.
– Object the effect of HBOT, TMS and EF in cortical functioning.
– Evaluate the effect of HBOT, TMS and EF on fatigue.
– Evaluate the effect of HBOT, TMS and EF on psychological aspects, such as depression and
anxiety.
– Evaluate the effect of HBOT, TMS and EF on the perception of pain and the number of
painful points.
– Evaluate the effect of HBOT, TMS and EF on the quality of sleep.
– Evaluate the effect of HBOT, TMS and EF on the quality of life.
– Evaluate the effect of HBOT, TMS and EF on the pain constructs.
– Determine the effect of HBOT, TMS and EF on plasma endorphin levels.
Heat Shock Protein 70 (HSP70) Reduces Hepatic Inflammatory and Oxidative Damage in a Rat Model of Liver Ischemia/Reperfusion Injury with Hyperbaric Oxygen Preconditioning.
Abstract: BACKGROUND Several clinical conditions can cause hepatic ischemia/reperfusion (I/R) injury. This study aimed to determine the mechanism of the protective effect of hyperbaric oxygen preconditioning (HBO₂P) on hepatic ischemia/reperfusion (I/R) injury in a...
Effect of hyperbaric oxygen therapy and corticosteroid therapy in military personnel with acute acoustic trauma.
Abstract: Acute acoustic trauma (AAT) is a sensorineural hearing impairment due to exposure to an intense impulse noise which causes cochlear hypoxia. Hyperbaric oxygen therapy (HBO) could provide an adequate oxygen supply. The aim was to investigate the effectiveness...