HBOT Conversations:
Tom Fox (Part 1)
Tom is the Research Physiologist for the Hyperbaric Institute for Research and Training, a division of Island Hyperbaric Centre in Pincourt QC. He has worked in the field of Clinical Hyperbaric Oxygen for the last 30 years, and has been intimately involved with the implementation and the development of the US Army’s Clinical Hyperbaric Service at Dwight David Eisenhower Army Medical Center. Tom is a senior army aviator and flew twelve years as a Medical Evacuation Pilot for the US Army.
Tom joined the Extivita-RTP team in 2022 as the Safety Director, and is joining us in a 2-part series to discuss the history of Hyperbaric Oxygen Therapy and dive into his personal experience healing patients with HBOT.
Watch the Podcast
We appreciate HBOT historian, Tom Fox, returning to HBOT News to dive in deeper to the history of Hyperbarics, which we can date back to the 1660s!
Tom explains that in the 1830s, the first clinical use of hyperbarics was used and introduced, this revived Nathaniel Henshaw’s concept of Hyperbaric treatments. Nathaniel Henshaw, a clergyman, built a sealed chamber in 1662. Henshaw believed that the application of higher pressure (hyperbaria) was good to treat acute conditions, and that lower pressure (hypobaria) would be better to treat chronic diseases.
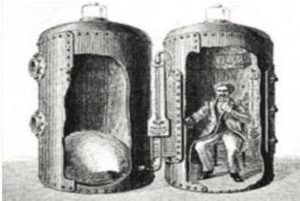
1662, Henshaw’s “Domicilium” hyperbaric chamber
This is an interesting fact, because now we’re learning that the cyclic use of hyperbaria (or relative hyperbaria) and hypobaria is very intriguing in what it’s doing from the standpoint of physiology. Tom mentions Dr. Efrati and his group of researchers have been at the forefront of looking at this, and are doing a phenominal job of conducting the hyperbaric studies and getting the hyperbaric education out there. There’s been very limited commitment to do this, he commends Dr. Efrati and his group at Tel Aviv for all they do for the HBOT industry. What you will witness throughout the history of hyperbarics is that they’ve used slightly pressurized room air, and that’s important to know because the slightly pressurized room air has consistently been assumed not to have any effect. It’s even offered up as a control in many of the studies, like the placebo. But the problem is when the placebo helps and the treatment helps, it’s easy to say that the reason both groups are getting better is because of the “participation effect”, or it being “in their heads”. And Dr. Efrati is bringing all this to light. This information is also changing the way the HBOT industry looks at the application of air breaks within the protocols. The use of air breaks was thought to fight oxygen toxicity, but now it’s used to establish a relative hypoxia without going into hypoxic conditions. Host di Girolamo then breaks all of that information down for the viewer to better understand…
So to paraphrase that, you’re breathing pure oxygen and also now you’re breathing air, your body says, ‘oh, oxygen’s depleting, you’re suffocating.’ All these mechanisms occur in your physiology, and then the body’s like, ‘Oh, no, everything’s okay. We have plenty of oxygen.’ So that five minute air break triggers that, and then he’s doing it, I think, three or four times in a 90 minute treatment and it ends up being therapeutic.
Continuing down the timeline of HBOT and fascinating discoveries in the 1800s, Tom Fox brings up a series of articles, Lectures on The Compressed Air Bath and its uses in the treatment of disease, that appeared in the British Medical Journal, dated April 18th, 1885 by a doctor, Theodore Williams. Tom reads the first paragraph from the first article:
“The use of atmospheric air under different degrees of barometric pressure in the treatment of disease is one of the most important advances in modern medicine. When we consider the simplicity of the agent, the exact method by which it is applied, and the precision with which it can be regulated to the requirements of each individual, we are astonished that in England, this method of treatment has been so little used.” – Theodore Williams
That was almost 150 years ago. Back then they were just taking air and putting you under pressure. Now it’s a breakthrough medical treatment, and it’s still not being used in the manner that it could/should be. Almost 200 years ago we were on the cutting edge of medicine! And today we still have to fight to explain that even slightly pressurized room air has a therapeutic benefit — using pressure for healing purposes has literally been happening since the 1600s.
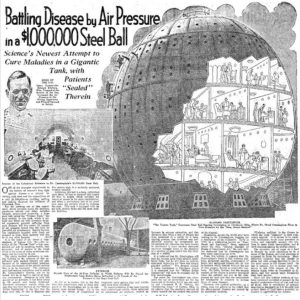 Now we approach the 1900s in the HBOT history timeline. One of the most famous (and LARGEST) chambers is discussed, the Cunningham Ball, by Dr. Cunningham. Dr. Cunningham clearly saw the benefits of Hyperbaric Oxygen Therapy and basically risked his entire career/life, and life savings to help people and prove the benefits. Doctor Cunningham was an anesthesiologist by trade, inventing circuits that are still in use and still patented by anesthesiology. In the 1918s, with the last pandemic of the Spanish Flu, Dr. Cunningham made the observation that there was a higher mortality rate when you went to Denver, as opposed to when you were at sea level, because of the pressure and oxygen changes. Ultimately a Spanish Flu patient in Denver was getting a lower dose of oxygen because of the lower air pressure. Dr. Cunningham even saved the life of one gentleman who was turning blue by simply treating with hyperbaric air. This lead to the dedication of $1M in funds to build the famous Cunningham ball, which was almost like a pressurized six story hotel that people would live in for a month or other extended periods of time.
Now we approach the 1900s in the HBOT history timeline. One of the most famous (and LARGEST) chambers is discussed, the Cunningham Ball, by Dr. Cunningham. Dr. Cunningham clearly saw the benefits of Hyperbaric Oxygen Therapy and basically risked his entire career/life, and life savings to help people and prove the benefits. Doctor Cunningham was an anesthesiologist by trade, inventing circuits that are still in use and still patented by anesthesiology. In the 1918s, with the last pandemic of the Spanish Flu, Dr. Cunningham made the observation that there was a higher mortality rate when you went to Denver, as opposed to when you were at sea level, because of the pressure and oxygen changes. Ultimately a Spanish Flu patient in Denver was getting a lower dose of oxygen because of the lower air pressure. Dr. Cunningham even saved the life of one gentleman who was turning blue by simply treating with hyperbaric air. This lead to the dedication of $1M in funds to build the famous Cunningham ball, which was almost like a pressurized six story hotel that people would live in for a month or other extended periods of time.
Apparently, Cunningham had some difficulty justifying it all by scientific standards, and this was a very new concept in US medicine. The world had never seen anything like it! Unfortunately, Cunningham fell victim toa unusual amount of scrutiny, and was eventually shut down with the chamber being sold for scrap metal during World War II.
So many people now see the value in Cunningham’s efforts and what he contributed to the HBOT industry. Finally, his work can be interpreted as vindication of the God-given miracle of oxygen and pressure to heal our bodies and minds.
Guests

Thomas M. Fox, MAS,MS, CHT - Safety Director at Extivita RTP & Research Physiologist for the Hyperbaric Institute for Research and Training
Tom is the Research Physiologist for the Hyperbaric Institute for Research and Training, a division of Island Hyperbaric Centre in Pincourt QC. He has worked in the field of Clinical Hyperbaric Oxygen for the last 30 years. During this time, he has been intimately involved with the implementation and the development of the US Army’s Clinical Hyperbaric Service at Dwight David Eisenhower Army Medical Center. He has provided contract hyperbaric services since 1997. Prior to accepting his current position in Quebec, Canada, Mr. Fox served as the Chief of the Atmospherics Branch of the U.S. Army School of Aviation Medicine, Fort Rucker Alabama. In this capacity, he was responsible for hyperbaric/ hypobaric operations and training of US and NATO aviators, flight surgeons and flight medics. Mr. Fox is a senior army aviator and flew twelve years as a Medical Evacuation Pilot for the US Army.
Tom joined the Extivita team in 2022 as the Safety Director, helping Extivita to maintain a healthy and safe environment for exceptional patient care.
Subscribe Now, It’s Free!
Recent HBOT News
Clinical Trial – 1% Chloroprocaine(PF) vs. Bupivacaine Spinals
The use of 1% Chloroprocaine (PF) spinal anesthesia will reduce the recovery times and
discharge time of patients undergoing hemorrhoidectomies as compared to 0.75% bupivacaine
spinal. The primary objective is to compare the recovery times (return of motor and sensory
function) and discharge time (voiding time) between 2-Chloroprocaine and 0.75% bupivacaine
spinal anesthesia for hemorrhoidectomies. This is a randomized, prospective study assigning
patients to either 2-Chloroprocaine (PF) or 0.75% bupivacaine spinal anesthesia group.
Clinical Trial – RCT of Epinephrine (None, 100mcg, and 200mcg) in a Hyperbaric Bupivacaine, Fentanyl and Morphine Spinal in C-sections.
This is a prospective, randomized, double blind study of 75 patients (n=25 for each group) in
which epinephrine (100mcg or 200mcg) or normal saline vehicle is added to intrathecal
hyperbaric bupivacaine (0.75% bupivacaine hydrochloride in 8.25% dextrose), fentanyl, and
morphine to prolong the duration of the spinal anesthetic in scheduled cesarean deliveries.
The primary outcome of duration will be the time to T10 level sensory regression as well as
motor level regression that will be graded via the modified Bromage scale.
Repeat cesarean sections, in particular, are associated with increased operative time and
thus often performed with a spinal-epidural (CSE) technique. The epidural component is,
however, untested and may not provide adequate anesthesia, thus the higher risk of conversion
to a general anesthesia. Epinephrine is routinely used to prolong spinal anesthesia. If
effective for the duration of a repeat cesarean section it would obviate the additional time
and risks of performing the epidural and still avoid sufficient duration to avoid conversion
to a general anesthetic.
Current treatment of central retinal artery occlusion: a national survey.
Central retinal artery occlusion (CRAO) is an ophthalmological emergency, the retinal analog of a stroke. To date there is no consensus or national guidelines on how this disorder should be managed. As academic neurologists and ophthalmologists treat CRAO frequently, we set out to understand how these clinicians approach patients with CRAO with a national survey. We identified university-associated teaching hospitals offering vascular neurology, neuro-ophthalmology and/or retina fellowships in the US and asked the directors of the programs to respond to questions in an open response format to profile the acute management of CRAO at their institution.